
Read AAPLOG Action Supports Repeal of 79
What happens in states that pass constitutional abortion amendments?
July 14, 2026
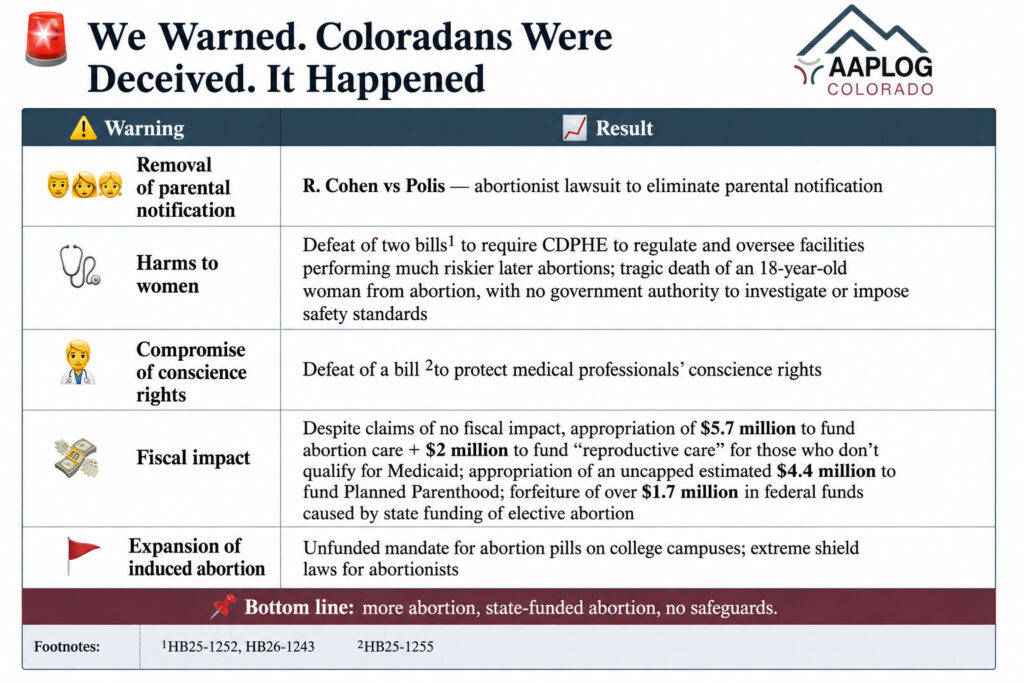
Harms of 79: warnings and fulfillment
In 2024, Harms of 79 warned that Amendment 79 would:
- Eliminate parental notification prior to a minor daughter’s abortion
- Prevent Coloradoans and their elected representatives in the legislature from enacting any restrictions on abortion late in pregnancy after the fetus could survive independently from her mother if born prematurely
- Strip the fetus of all legal value and protections and prevent professional medical organizations or state government from regulating abortion methods and prohibiting especially cruel abortion procedures
- Make the state unable to establish or enforce prudent health and safety standards pertaining to second and third trimester abortion clinics. Patients’ health and lives will continue to be jeopardized
- Compromise the conscience rights of physicians, nurse practitioners, and nurses
The 2024 Colorado Voter’s Guide Fiscal Impact section for Amendment 79 begins, “The measure will have no fiscal impact to state and local governments, as it places current 16 state law and practices around abortion services into the Colorado Constitution.” However, the amendment included the repeal of Amendment 3, the prohibition of using tax payer dollars to fund elective abortion through Medicaid and government employee insurance.
What has happened in Colorado since Amendment 79 passed?
Parental notification: Dani Newsum, the director of COBALT, which was one of the primary sponsors of Amendment 79, claimed publicly that the Amendment had “nothing to do with parental notification.” (Timestamp 7:19)
However abortionist Rebecca Cohen has filed legal action against Colorado to remove parental notification of a minor daughter’s abortion, claiming it is unconstitutional under Amendment 79.
The Colorado legislature in 2026 went one step further, expanding the definition of abuse in custody decisions: “Health-care abuse” – “Interference with or controlling or preventing access to reproductive healthcare, including contraceptive use or reproductive health care information, or controlling or attempting to control reproductive outcomes…” It also added “coercive control” to the definition of abuse, including monitoring their child’s “access to services…” (HB26-1309).
Safeguards for women: defeat of CDPHE regulation of later abortion facilities
The Colorado legislature has twice defeated bills to require similar regulation, oversight and licensure of abortion facilities that perform the increasingly more dangerous second and third trimester abortions, as required for facilities that perform similarly or less-risky procedures, such as Ambulatory Surgery Centers and free-standing Birth Centers (HB26-1243 and HB25-1252). Since the passage of Amendment 79, an 18 year-old woman died of complications from a late second trimester abortion. The Colorado Department of Health and Education has no authority to investigate, or to require improvements in care that may save future women’s lives. 90% of maternal deaths (which include deaths from abortion in Colorado) are preventable; but Colorado protects abortionists, not women.
Conscience Protections for Medical Professionals
In 2025, the Colorado legislature defeated a bill to protect the conscience rights of medical professionals (HB25-1255).
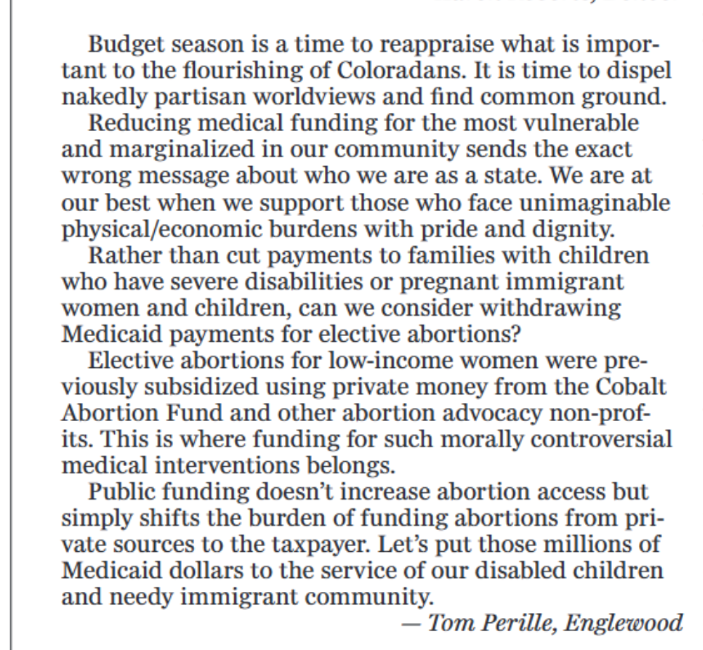
Cost to Tax Payers
Despite the assurance of no fiscal impact, the Colorado legislature immediately passed legislation to use public funds for elective abortion (euphemized as “certain pregnancy related services”) through Medicaid and government employee insurance (SB25-183). The fiscal note for the bill claimed an eventual cost savings to fund elective abortion by “averted births,” both immediate “savings” and decreased need for the “safety net.” “Medicaid-covered births typically involve additional social safety net costs for the child, whereas abortion care services represent a one-time expenditure.” “No fiscal impact” became: “For FY 2025-26, the bill requires and includes the following appropriations to the Department of Health Care Policy and Financing:
- an increase of $1,476,896 from the General Fund;
- a decrease of $41,650 from the Healthcare Affordability and Sustainability Fee Cash Fund; and
- a decrease of $1,721,497 from federal fund (forfeiture of federal funds caused by state funding of elective abortion.”
During the special session called in August 2025 to address the state budget deficit of nearly $1 Billion, the Colorado legislature determined to fund Planned Parenthood, euphemistically called “State-Only Funding for Certain Entities” (SB25B-002). The fiscal note estimated up to nearly $4.4 Million appropriations of public monies, although there is no cap in the bill.
The full fiscal impact of Amendment 79 is yet to be realized, but the 2026-2027 appropriations budget includes $5.7 Million for abortion care, and an additional line item of $2 Million for “Reproductive Health Care for Individuals Not Eligible for Medicaid.” Abortion funding was prioritized over other essential healthcare services, which were cut, including benefits for pregnant women through Cover All Coloradans, reductions in provider reimbursement, long-term services and supports, disability waiver programs, family caregiver payments, and other Medicaid services.
Mandated Abortion Pill Provision on college campuses
In 2026, the Colorado legislature passed an unfunded mandate requiring campuses that have a health clinic to stockpile and dispense abortion drugs (HB26-1335). Again, there is an unexplainable fiscal note of zero. However, in California, the only other state with a requirement for abortion provision on campuses, $200,000 was provided to each campus for implementation; ongoing cost of provision are not yet reported. Colorado’s mandate has no provision for standards of medical care, emergency access to medical care for complications, nor data collection for quality and cost.
In the same legislative session, HB26-1141 changed the definition of harassment and discrimination on education institutions campuses from kindergarten through higher education to: “”Harassment or discrimination” means to engage in, or the act of engaging in, any unwelcome physical or verbal conduct or any written, pictorial, or visual communication by a student or employee that is directed at a student or group of students because of that student’s or group’s membership in, or perceived membership in, a protected class….” Protected classes were expanded to include pregnancy and parenting status. Data and grievance procedures will be publicly available. This bill potentially chills groups on college campuses that may offer other pregnancy options to pregnant college women, while HB26-1335 mandates one option – abortion.
Coloradans were duped! When the amendment sponsors incorporated language that nothing shall deny, impede or restrict access to abortion, they meant it… and more. Free abortion for all with no restrictions or protections for women or minors.
Read the full “Harms of 79” declaration below.





{kind=link}